Health Outcome Studies
“Natural forces within us are the true healers of disease.”
An estimated 60% to 80% of primary-care doctor visits are related to stress.[60-62] HeartMath’s easily learned mental and emotion self-regulation techniques and practices can provide an effective strategy for stress reduction in many clinical contexts. As discussed earlier, these intentionally simple techniques allow people to quickly self-induce a physiological shift to a more coherent state that takes advantage of the concurrent change in afferent neuronal input to the brain, which is associated with increased self-regulatory capacity and thus, ability to more successfully handle the demands and challenges of life with more ease and composure. Consequently, there is a greater experience of connectedness, harmony, balance and physical, emotional and psychosocial well-being.
HeartMath interventions have facilitated health improvements in patients with:
- Hypertension
- Arrhythmias
- Autoimmune disorders
- Environmental sensitivity
- Sleep disorders
- Drug and alcohol addiction
- Anger
- Heart failure
- Chronic pain
- Fibromyalgia
- Chronic fatigue
- Anxiety disorders
- Depression
- PTSD
- ADD/ADHD
- Eating disorders
Health-care professionals worldwide, representing both mental health and medical fields, are incorporating HeartMath self-regulation techniques and practices into their treatment strategies with notable success. A growing number of clinical studies and case histories have documented substantial reductions in symptomatology and improvements in clinical status in a wide variety of conditions after a relatively brief time when their patients use these techniques and practices. Collectively, results indicate that such self-regulation techniques are easily learned and employed, produce rapid improvements, have a high rate of compliance, can be sustained over time and are readily adaptable to a wide range of age and demographic groups.
The use of interventions utilizing the HeartMath selfregulation techniques and HRV coherence feedback technology to reduce stress has significantly improved key markers of health and wellness. For example, studies have shown the use of these self-regulation techniques increases parasympathetic activity (HF power) [133] and results in significant reductions in cortisol and increases in DHEA (Figure 8.1) over a 30-day period [116]. In a study for which results are shown in the figure, 30 participants were taught the Cut-Thru and Heart Lock-In self-regulation techniques and practiced using them in daily life for one month. The significant changes in hormonal balance correlated with the significant improvements in emotional health and reductions in stress, anxiety, burnout and guilt along with increases in caring and vigor.
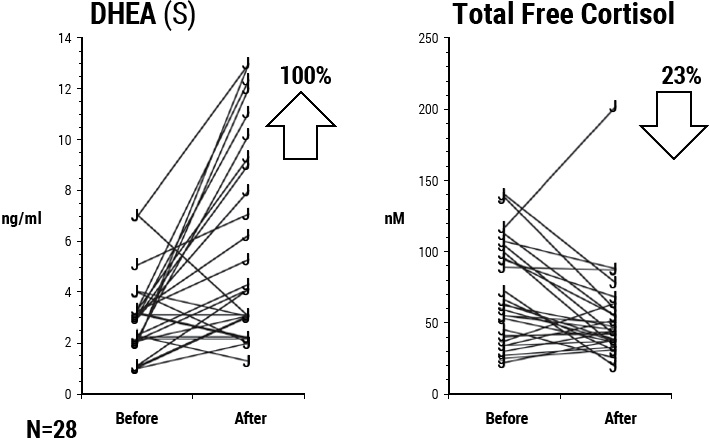
Figure 8.1 DHEA and cortisol values before and after subjects were trained in and practiced HeartMath self-regulation techniques for one month. There was a 100% average increase in DHEA and a 23% decrease in cortisol.
Coherence and Blood Pressure
Several studies have shown significantly lowered blood pressure (BP) and stress measures. Employees with a diagnosis of hypertension who were enrolled in a workplace-based risk-reduction program exhibited significant reductions in blood pressure relative to the control group after using HeartMath tools for three months.[115] Participants also experienced significant reductions in distress and depression, concurrent with improvements in work performance-related parameters following the intervention (Figure 8.2).
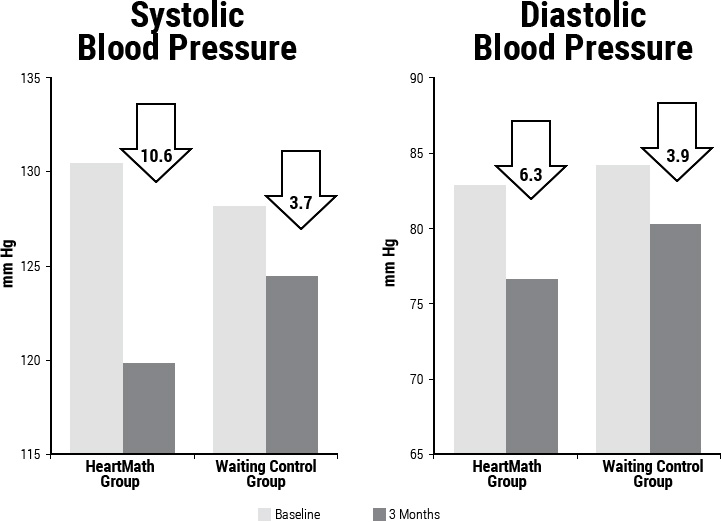
Figure 8.2 Changes in systolic and diastolic blood pressure in the HeartMath group versus the control group. BP was measured before and three months after the completion of the training program. The trained group demonstrated a mean adjusted reduction of 10.6 mm Hg in systolic BP and of 6.3 mm Hg in diastolic BP. (Three-month measurements are adjusted for baseline BP, age, gender, body mass index and medication status.) *p < .05.
The trained group demonstrated a mean adjusted reduction of 10.6 mm Hg in systolic BP and of 6.3 mm Hg in diastolic BP, as compared to reductions of 3.7 mm Hg (systolic) and 3.9 mm Hg (diastolic) in the control group. In addition, three individuals in the trained group were able to reduce their BP medication usage, with their physicians’ approval, during the study period. Of these, one participant was permitted to discontinue antihypertensive medication usage entirely following completion of the study. These BP improvements achieved by the treatment group are notable when viewed in comparison to BP reductions typically achieved with other types of interventions. The reduction in BP obtained through the stressmanagement training is similar in magnitude to the average reduction in BP reported in a meta-analysis of controlled trials of anti-hypertensive drug therapy that lasted for several years. This reduction in BP is the equivalent of a 40-pound weight loss, and is twice the size of the average reduction seen with, for example, a low-salt diet or exercise training.[263-265]
In another study of hypertensive patients, it was found that those who used the techniques to increase HRV coherence had rapid reductions, on average, of 10mm Hg in mean BP. The study was a randomized controlled design with 62 hypertensive participants who were divided into three groups. (Group 1 participants were taking hypertensive medications and taught the Quick Coherence self-regulation technique and used a heart rate variability (HRV) coherence-training device. Group 2 members were not yet taking medications and were trained in the Quick Coherence Technique; those in Group 3 were taking hypertensive medications and did not use the Quick Coherence Technique, but instead were instructed in a relaxation technique that they used between the BP assessments. An ANCOVA (analysis of covariance) was conducted to compare the effectiveness of three different interventions at reducing blood pressure. The two groups that used the Quick Coherence self-regulation technique and HRV coherence-training device were associated with a significantly greater reduction in systolic and mean arterial pressure (average blood pressure) compared with the medication/relaxation technique-only group. The greatest reductions in blood pressure were associated with the combination of medications and the use of the HRV coherence device and the self-regulation technique. Surprisingly, the group that was not taking medications had greater reductions than the medications/ relaxation group (Figure 8.3).[113]
Health Risk Reduction in Correctional Officers
A study of 88 California correctional officers with high workplace stress was randomized to experimental and wait-list control groups, stratified on relative health risk, age and gender.[266] The experimental group participated in a stress- and health-risk reduction program, which was delivered over two consecutive days.
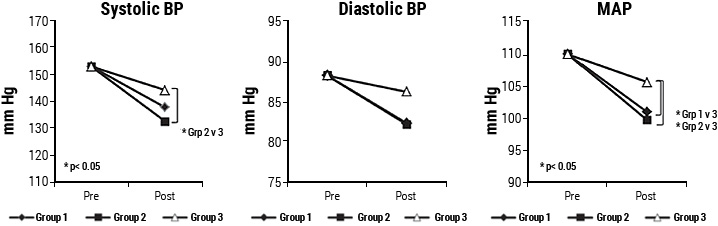
Figure 8.3 Shows the pre-post intervention changes in systolic, diastolic and mean arterial blood pressure for the three groups. The use of the Quick Coherence self-regulation technique and HRV coherence-training device was associated with a significantly greater reduction in systolic and mean arterial pressure (average blood pressure) in the two groups who used the intervention compared with the medication/relaxation technique-only group. The greatest reductions in blood pressure were associated with the combination of medications and the intervention using the HRV device and self-regulation technique.
The program included instruction on health-risk factors as well as training in HeartMath’s self-regulation techniques. Learning and practice of the techniques were enhanced by HRV coherence feedback. Physiological changes in the experimental group included significant reductions in total cholesterol, LDL cholesterol levels, the total cholesterol/HDL ratio, fasting glucose levels, mean heart rate, mean arterial pressure, and both systolic and diastolic blood pressure (Figure 8.4).
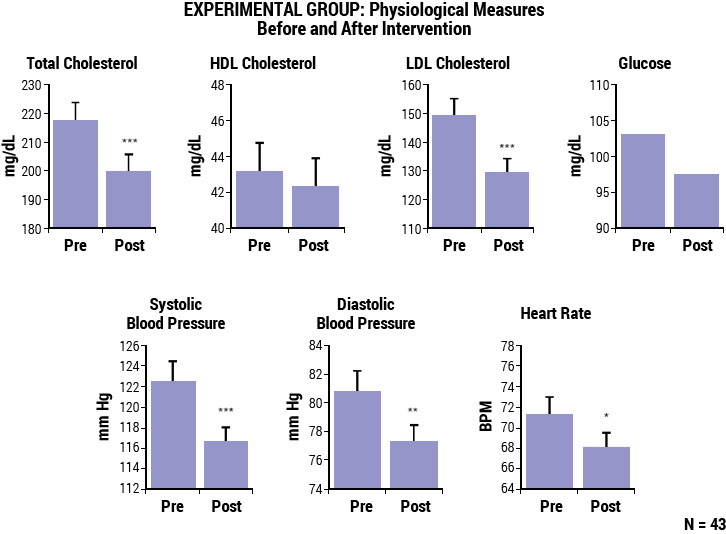
Figure 8.4 Bar graphs illustrate physiological variables in the experimental group, measured before and three months after the intervention program. The group showed significant reductions in total cholesterol, LDL cholesterol, blood glucose levels, systolic and diastolic blood pressure, and heart rate after the intervention. *p < 0.05, **p < 0.01, ***p < 0.001.
Psychological changes included significant reductions in overall psychological distress, anger, fatigue, hostility, interpersonal sensitivity, impatience, and global Type A behavior, and increases in gratitude and positive outlook. There were also improvements in key organizationally relevant measures in the experimental group after the program, including significant increases in productivity, motivation, goal clarity and perceived manager support. Finally, a detailed analysis was performed to calculate the projected health-care cost savings to the organization that would likely result from the reduction in participants’ health risk factors. According to this analysis, the reductions in health-risk factors achieved in this study were projected to lead to an average health-care cost savings of $1,179 per employee per year.
Health-Care Cost Reduction
The Reformed Church in America (RCA) identified stress among its clergy as a major cause of higher-than-average health claims. Because the pastors were spread across the U.S., the intervention was provided by a small team of HeartMath certified mentors in six phone sessions to help the participants manage stress and increase physiological resilience. The study divided 313 participants into two groups with 149 participating in the HeartMath program delivered by phone, which included instruction in use of the portable version of the emWave and practice of the self-regulation techniques and 164 in the active control group participated in a phone-based lifestylemanagement program. All participants completed a health-risk assessment and a validated HeartMath Personal Well-being Survey at the beginning of 2007 and again at the beginning of 2008. Well-being, stress management, resilience, and emotional vitality were significantly improved in the HeartMath group compared to the lifestyle-management group. In an analysis of the claims costs data for that year, the pastors who had participated in the HeartMath program were compared to the control group. Adjusted medical costs were reduced by 3.8% for HeartMath participants while there was an increase of 9.0% for the control group. The adjusted pharmacy costs increased 7.9% for the HeartMath group and 13.3% for the control group. The total 2008 savings as a result of the program were $585 per participant, yielding a return on investment of 1.95:1. In the detailed medical cost analysis, one of the higher cost-savings categories was for essential hypertension, which would be expected to be sensitive to reduced stress.[112]
Metabolic Syndrome
A number of significant health outcomes were found in two workplace pilot studies of utility line workers and employees of an online travel company. These studies focused on reducing stress and metabolic syndrome risk factors with the HM self-regulation techniques combined with HRV coherence feedback. In both studies, there were significant reductions in organizational stress (life pressures, relational tensions, work-related stress), emotional stress (anxiety, depression, anger) and stress symptoms (fatigue, sleep, headaches, etc.), and significant increases in emotional vitality. Both studies also showed reductions in the number of participants who were classified as having metabolic syndrome. In the utility-company cohort, total cholesterol and LDL cholesterol were significantly reduced, and the travel-company cohort had significant reductions in both systolic and diastolic BP and triglycerides (unpublished data).
Asthma/Pulmonary Function
One of the reasons coherence training is an effective approach for reducing both short-term and long-term BP, may be a resting of baroreflex gain. Psychophysiologist Paul Lehrer, has shown that using HRV feedback to promote a state of physiological coherence, which he calls "resonance," resulted in lasting increases in baroreflex gain, independent of respiratory and cardiovascular changes.[111] In a large controlled study involving patients with asthma, those using the HRV resonance training had improved lung function, decreased symptoms, exhibited no asthma exacerbations and were able to reduce steroid medications.[267] In other studies, Lehrer demonstrated that pulmonary function improvements occurred in both older and younger patients even though older individuals have lower HRV[183] and that the improvements occur with HRV biofeedback training, but not with relaxed breathing or muscle tension relaxation.[268] He also published a report of 20 case studies which showed uniform improvements in pulmonary function in children with asthma.[269] Additionally, according to Lehrer, in a controlled study, patients with multiple unexplained symptoms and depression[270] showed improvements, as did patients with fibromyalgia[271] and major depression.[272]
Congestive Heart Failure
A study was conducted at Stanford University to evaluate the effect of the HeartMath self-regulation skills training on quality of life and functional capacity in elderly patients with class I-III congestive heart failure (CHF).[192] Thirty-three multiethnic patients (mean age, 66±9 years) were randomly assigned to a treatment group or wait-listed control group. The intervention was provided in eight weekly sessions over a 10-week period. Significant improvements were noted in perceived stress, emotional distress, six-minute walk and depression, and positive trends were noted in each of the other psychosocial measures. The investigators noted that CHF patients were very willing participants and the study suggested that HeartMath techniques were a feasible and effective intervention for CHF patients, demonstrating that stress and depression levels could be reduced and functional capacity increased in this population through training in emotion self-management. This study’s promising indications clearly warrant larger-scale controlled trials to confirm the observed psychosocial and functional improvements and further explore the implications of such outcomes for physiological rehabilitation (Figure 8.5-8.7).
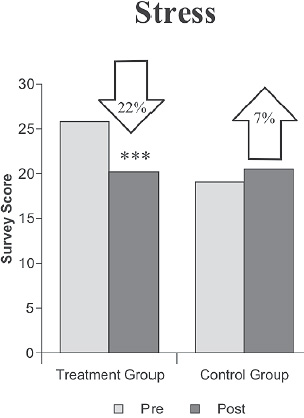
Figure 8.5 Reduction in stress in congestive-heart-failure patients after the HeartMath training program. Stress dropped 22% in the treatment group following the intervention, while it rose 7% in the control group over the three-month study period. (Perceived Stress Scale) ***p < .001.
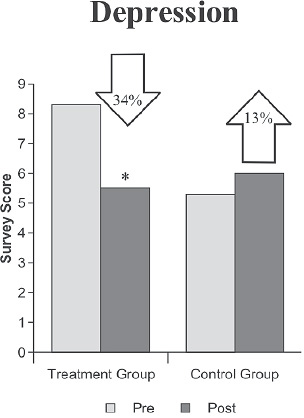
Figure 8.6 Reduction in depression in congestive-heart-failure patients after the HeartMath training program. Depression decreased by 34% in the treatment group whereas it increased by 13% in the control group over the study period. (Geriatric Depression Scale) *p < .05.
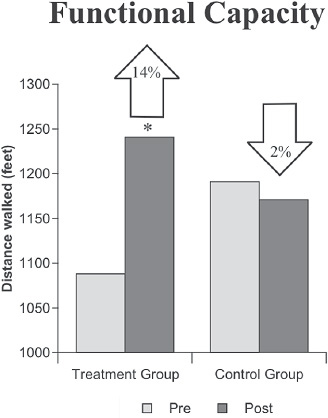
Figure 8.7 Improvements in functional capacity in congestive-heart-failure patients after the HeartMath program. Functional capacity, as measured by performance on the six-minute walk, increased 14% in the treatment group while it declined 2% in the control group. Treatment-group participants were able to walk an average of 153 feet further in six minutes at posttest than at pretest. *p < .05.
Diabetes
In a study of diabetes patients, the introduction of the self-regulation skills led to an improved overall quality of life and glycemic regulation, which correlated with use of the self-regulation techniques.[273] Twenty-two patients with Type 1 or Type 2 diabetes mellitus participated in a two-day training. Hemoglobin A1c, cholesterol and triglycerides, and blood pressure were assessed along with measures of stress, psychological status and quality of life before and six months following the training. There were significant reductions in psychological symptomatology and negative emotions, including anxiety, depression, anger and distress and significant increases in peacefulness, social support and vitality, as well as reductions in somatization, sleeplessness and fatigue.
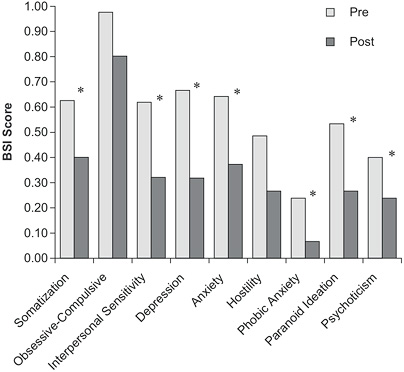
Figure 8.8 Diabetic patients demonstrated significant reductions in a numerous psychological symptoms (Brief Symptom Inventory) after practicing the HeartMath interventions for six months. *p < .05.
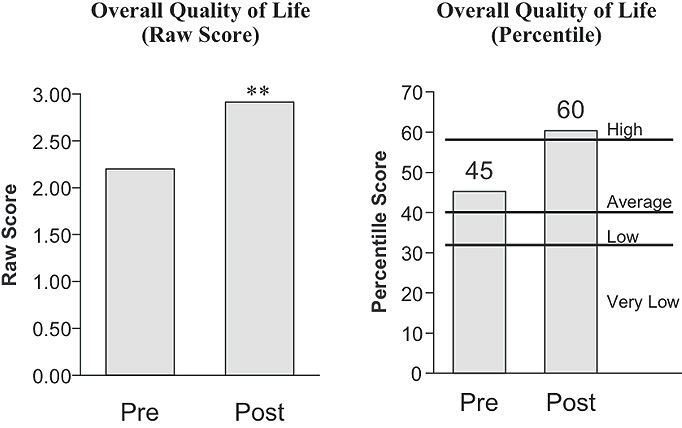
Figure 8.9 The graph on the left illustrates the significant increase in the group’s mean overall quality of life raw score, as measured by the Quality of Life Inventory three weeks before versus six months after the HeartMath program. The graph on the right plots the mean overall quality of life percentile score for study participants as compared to normative data. Before the intervention program, the group’s mean percentile score plotted very near the bottom of the average range, whereas six months after the program it had moved into the high range. **p < .01.
Participants also showed reduced sensitivity to daily life stressors, and quality of life significantly improved (Figures 8.8 and 9). Regression analysis revealed a significant relationship between self-reported practice of the techniques learned in the program and the change in HbA1c levels in patients with Type 2 diabetes with more practice being associated with reductions in HbA1c.
Coherence and Improved Cognitive Function
Several studies have shown that increased levels of heart-rhythm coherence are associated with significant improvements in cognitive performance.[5, 108, 109] Significant outcomes have been observed in discrimination-and reaction-time experiments and more complex domains of cognitive function, including memory and academic performance.[5, 274] In terms of healthier cognitive and emotional functioning, significant reductions in stress, depression, anxiety, anger, hostility, burnout and fatigue, and increases in caring, contentment, gratitude, peacefulness, resilience and vitality have been measured across diverse populations.[275-280]
Attention Deficit Hyperactivity Disorder (ADHD)
ADHD, the most commonly studied and diagnosed behavioral condition in childhood, is estimated to affect 3% to 5% of children globally. Left untreated, ADHD can lead to academic underachievement, poor interpersonal relationships, anxiety, depression and increased risk of criminal activity. Of particular concern is the increased risk of mental health problems for adolescents with ADHD.
A randomized blind, placebo-controlled study was undertaken with 38 children (aged 9 to 13) with a clinical diagnosis of ADHD in Liverpool, England to assess the potential benefits of HeartMath self-regulation techniques. Learning the skills was supported by HRV coherence feedback training. The placebo control consisted of daily 20-minute, one-on-one sessions with a learning assistant for six weeks. During these sessions, each child was free to build a model of choice from Lego building blocks. Cognitive function was assessed using a comprehensive set of computer-based tests of attention, concentration, vigilance, short-term (working) memory and long-term (episodic) memory before the intervention and again six weeks later. Secondary measures included the Conners’ Teachers Rating Scale and the Strengths and Difficulties Questionnaire completed by both children and their teachers. After the post-intervention measures were collected, the control group was provided with the same HeartMath self-regulation skills program. Participants demonstrated significant improvements in various aspects of episodic secondary verbal memory, including delayed word recall and immediate word recall and word recognition (Figure 8.10). Significant improvements in behavior also were found. The results suggest that the intervention offers a physiologically based program to improve cognitive functioning and behaviors in children with ADHD.[108]
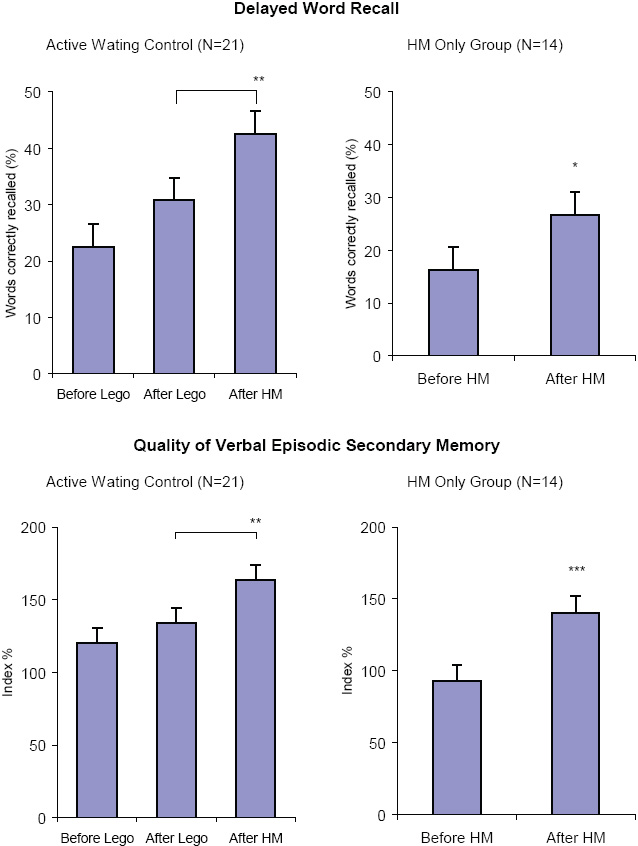
Figure 8.10 Children with ADHD in the HeartMath group exhibited significant increases in overall quality of episodic memory and long-term memory. Children in the placebocontrol group (Lego play) showed a small, but non significant improvement over the same time period. There was a significant improvement in the control group as well after they learned and practiced the HeartMath skills. Quality of verbal episodic memory is a composite measure constructed from accuracy measures of four cognitive function tests. * p < 0.05, ** p < 0.01, *** p < 0.01.
Improved Mental Health in Children
A study conducted by the Department of Psychophysiology at an outpatient pediatric clinic in Skopje, Macedonia evaluated the effectiveness of HRV coherence training and the HeartMath self-regulation techniques in the treatment of common mental health disorders in children.[281] Six groups of children were evaluated: a) children with anxious phobic symptoms, N = 15, mean age 12.5 ± 2.25 years; b) children with somatoform problems (somatic symptoms not explained by a general medical condition), N = 15, mean age 10.92 ± 2.06; c) children with obsessivecompulsive manifestations (OCD), N = 7; mean age 14.5 ± 2.20; d) children with ADHD, N = 10, mean age 10.5 ±.1.80; e) children with conduct disorders (CD), N = 12, mean age 11.5 ± 1.52; and f) a control group, N = 15 children, mean age 10.18 ± 1.33. All of the examined children (N = 74) were of similar age. The diagnosis was made according to ICD-10 classification by a team of pediatrician-psychophysiologists, a clinical psychologist and a child neurologist. All children were outpatients at the Skopje pediatric clinic. In the assessment procedure, interviews with parents and children and psychometric evaluations with the Eysenck Personality Questionnaire (EPQ) were used to discriminate four main psychological personality characteristics: extroversion/introversion; neurotic tendencies/stability; psychopathologic traits/normal behavior; and self-control/lie scale.
The biofeedback instrumentation used was HeartMath’s HRV coherence-training system (Freeze-Framer, now called emWave Pro). It was used to reinforce the self-regulation techniques. Each patient sat in a comfortable chair in a quiet room with the practitioner. Patients were instructed to practice a self-regulation technique that included rhythmic heart-focused breathing and to activate a positive emotion. After the initial assessment, 15 training sessions were provided. The duration of all sessions was about 16 minutes and included playing two games (Meadow and Balloon), which are controlled by the subject’s heart-coherence level.
The results were statistically elaborated with: ANOVA (analysis of variance) for the first and last sessions of all groups and Student t-test for differences between groups. Generally, all children manifesting mental health problems showed lower scores for extroversion and higher scores for neuroticism, compared to the control group at baseline. This finding was considered important in the choice of biofeedback modality. Namely, for introvert personalities, manifesting socalled "inner arousal," the application of peripheral biofeedback modalities was considered to be a better choice. In this context, peripheral biofeedback based on HRV coherence was chosen for the study.
It was found in the results analysis that significantly lower heart rate between the first and last session were obtained for obsessive-compulsive and conduct disorders and anxiety. It means that with training, almost all children, except the ADHD group, learned to lower their heart rate. The Anxiety group showed very good results related to HRV; they were able to increase HRV coherence scores. For children with somatoform problems, there also were significant increases in HRV parameters (VLF, LF and HF power). Changes in HRV in the OCD group also had significant increases in all HRV measures, which were considered to be an important clinical outcome. The children with ADHD did not have increased HRV. The coherence scores increased in all training sessions for all groups, but the highest increases were in the conduct disorder group followed by the general anxiety group (32.5 and 30 respectively). It also improved significantly in the OCD and somatoform disorders groups. HRV training showed very positive results relative to clinical outcomes, especially for children with conduct and anxious-phobic disorders, and for obsessive-compulsive and somatoform disorders.
In general, the authors concluded that HRV coherence training, as a peripheral biofeedback modality, could be a good noninvasive choice, especially for introverted children manifesting common mental health problems, and that the approach has a good cost-benefit ratio. The games included in the training are very engaging for children.
Coherence Training Improves Memory
In a study conducted by Keith Wesnes in London, 18 healthy adult participants (six females, 12 males, ages 20 to 53, mean 32 years) were recruited for a study to assess the potential long-term effects of HeartMath self-regulation skills and HRV coherence training on cognitive performance.[282]
Cognitive function was assessed using a comprehensive set of computer-based tests for attention, concentration, vigilance, short-term (working) memory and long-term (episodic) memory before the intervention and again seven weeks later. Each participant’s ECG was recorded for a 10-minute period for HRV and coherence analysis before administration of the cognitive function test battery. In addition, participants completed a short self-administered questionnaire that measured calmness and alertness. After baseline collection, the participants attended a training program in which they learned the Freeze Frame, Heart Lock-In, and Coherent Communication techniques, and instruction in using the HRV coherence feedback system (Freeze-Framer, now called emWave Pro). They were asked to use the Freeze Frame Technique whenever they experienced stress or emotional discord, and the Heart Lock-In Technique three times per week for at least 10 minutes. In addition, they were encouraged to practice the Coherent Communication Technique when engaging in conversation with others. Seven weeks later the participants completed the same measures using exactly the same protocols as were used and followed for baseline data collection.
The results of the pre- and post-analysis of the cognitive performance tests showed significant improvement (p = 0.0049) in the quality of episodic (long-term) memory and marginally significant improvement (p = 0.078) in the quality of working (short-term) memory (Figure 8.11). There was a positive trend in the composite scores reflecting the ability to pay attention and the speed with which they were able to retrieve information from memory. However, the improvements in these measures did not quite reach statistical significance. Analysis of the questionnaire data showed that the research participants reported feeling significantly calmer at the end of the study than they did at the beginning (t-test 2.44, p < 0.05). This finding is notable, in that Dr. Wesnes reported the magnitude of the improvement was significantly higher than the improvement in quality of memory obtained in a large clinical 14-week trial of the effects of a phytopharmaceutical memory enhancer (a gingko/ginseng combination) on the memory of healthy volunteers.
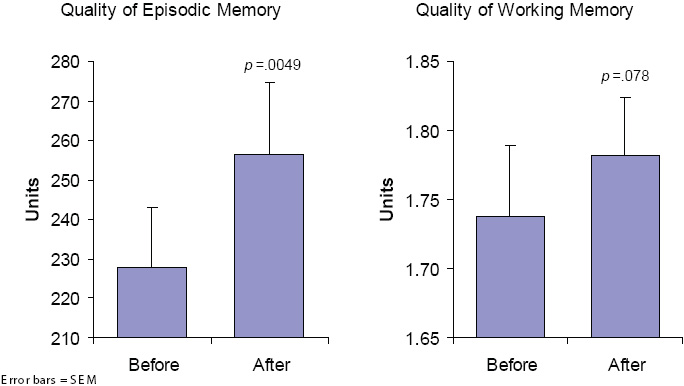
Figure 8.11 Mean improvements in quality of episodic (longterm) memory and quality of working (short-term) memory after participants practiced HeartMath coherence-building tools for seven weeks.
For HRV analysis, standard time and frequency domain HRV measures and coherence levels were computed. In relation to baseline measurement, a significant increase in heart-rhythm coherence (p < 0.001) was observed post-intervention before the participants were administered the cognitive function assessments. The group’s mean HRV power spectra showing the pre-post differences are shown in Figure 8.12. The increase in power around the 0.1-hertz frequency range indicates a pronounced increase in heart-rhythm coherence, and it occurred even though the participants were not specifically instructed to use any of the tools they had learned in the program.
In an effort to explain the observed pre-post changes in the quality of episodic memory and in self-rated calmness, two additional stepwise multiple regressions were run. Of the 10 independent variables included in each analysis, improvement in coherence was the only variable with sufficient statistical power to meet the criterion for entry into the stepwise analysis.
The results show that the change in coherence is quite strongly related to the observed changes in episodic memory and calmness: it accounted for 21% of the variance in the improvement in long-term memory and 42% of the variance in the reported increase in calmness.[5]
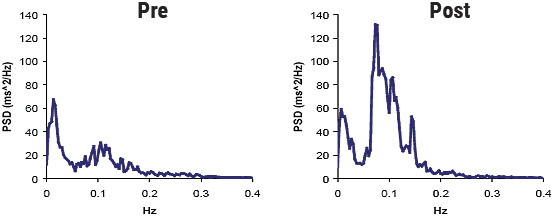
Figure 8.12 Group mean HRV power spectra calculated from 10-minute ECGs recorded before subjects completed the cognitive performance assessments. The left-hand graph shows the mean HRV power spectrum before participants were trained in the HeartMath self-regulation techniques, while the right-hand graph shows the mean power spectrum after they learned and practiced the techniques for seven weeks. Note the increase in power around the 0.1-hertz frequency range, indicating a pronounced increase in heart-rhythm coherence. This shift is particularly notable, as subjects were not specifically instructed to use the techniques during the post-recording.
Self-Regulation, PTSD Chronic Pain and Brain Injury
While overall health and wellness benefits have been associated with increased coherence, there is also evidence related more specifically to high-stress populations. A study at the William Jennings Bryan Dorn Veterans Affairs Medical Center in Columbia, S.C. of recently returning soldiers from Iraq who were diagnosed with PTSD, found that relatively brief periods of cardiac coherence training combined with practicing the Quick Coherence Technique resulted in significant improvements in the ability to self-regulate and significant improvements in a wide range of cognitive functions, which correlated with increased cardiac coherence. The study also found that resting HRV data in those with a PTSD diagnosis had lower levels of HRV and lower levels of coherence than control subjects without PTSD. Figure 8.13 shows the changes in cognitive function measures, and Figure 8.14 is an example of the typical changes in the HRV waveforms and power spectra from one of the participants.[109]
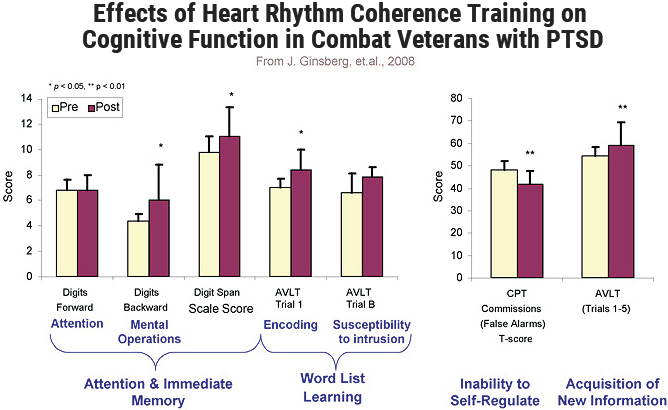
Figure 8.13 Improvements in various measures of cognitive function in recently returned combat veterans with PTSD, after learning the Quick Coherence self-regulation technique and receiving heart-rhythm coherence feedback training using the emWave Pro. Cognitive improvements co-occurred with increases in heart-rhythm coherence and overall HRV. * p < 0.05; ** p < 0.01.
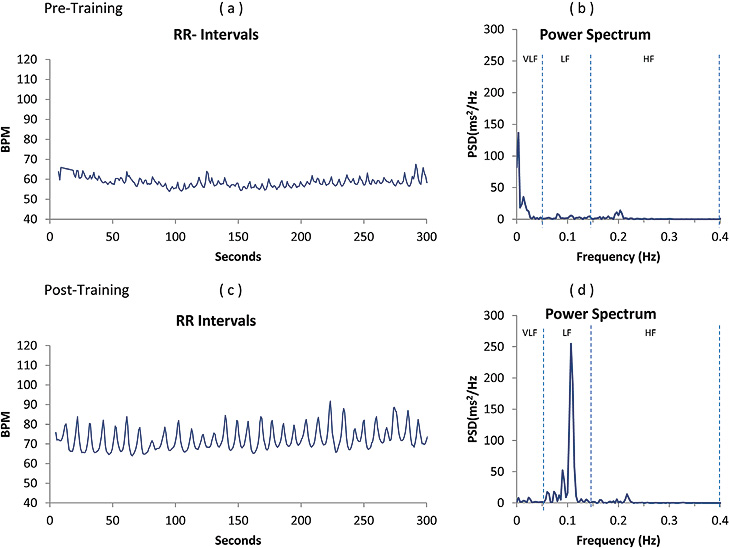
Figure 8.14 (a) and (b) depicts the pre-and post-HRVB Training the R-R interval tachogram and power spectra density of one subject with PTSD. Typical example of one of the participant’s HRV and power spectra: (a) HRV wave recording pre-training. (b) Power spectrum of HRV. (c) HRV recording post-coherence feedback training. (d) Power spectrum.
In a study of patients with severe brain injury, it was found that the emotion self-regulation training combined with HRV coherence feedback resulted in significantly higher coherence ratios and higher attention scores. Additionally, the families’ ratings of participants’ emotional control correlated with improved HRV indices.[283]
In a study of returning veterans with chronic pain, pre- and post-measurements of HRV, HRV variables, cardiac coherence, perceived pain, stress, negative emotions and physical activity limitation were made for both treatment and control groups. The treatment group received instruction in the Quick Coherence selfregulation technique, which incorporates controlled breathing and the self-induction of a positive or neutral emotion, along with the HRV coherence feedback device. The technique was practiced during four weekly biofeedback training sessions and was followed by a post-training assessment of pain, stress, and HRV. Control participants simply returned to the lab for a follow-up evaluation four weeks after the initial assessment. The treatment group showed marked and statistically significant increases in coherence (191%) along with significant reductions in pain ratings (36%), stress perception (16%), negative emotions (49%) and physical activity limitations (42%).[284]
Another study conducted in an outpatient pain rehabilitation clinic in a university hospital rehabilitation center in the Netherlands examined the benefits of adding the HeartMath self-regulation and HRV coherence training to a back school (BS) program for patients with chronic, nonspecific low back pain to explore the possible moderators of treatment success.[285] The secondary objective was to test the relationships between HRV coherence at discharge with pain, disability and health perception. It was hypothesized that higher change in coherence scores would be related to changes in pain, disability and health perception.
A total of 170 patients with chronic, nonspecific low back pain were enrolled in the study. Of these, 89 patients were assigned to the standard back school (BS) program and 81 were assigned for BS and heartcoherence training (BS+HCT). Inclusion criteria were: nonspecific lower back pain lasting at least three months and age 18 or older. Exclusion criteria were: mental (e.g. major psychiatric disorders) or physical causes (e.g. cardiac or pulmonary disorders or use of heart medication) or being currently treated for such. A rehabilitation physician approved each participant’s inclusion.
At baseline assessment before treatment (T0) and at discharge (T1), the patients filled out a comprehensive set of questionnaires, including demographics, the Pain Disability Index (PDI), the Roland Morris Disability Questionnaire (RMDQ), Numeric Rating Scale (NRS pain) and the RAND 36. HCT was evaluated using a standardized test procedure before HCT and at discharge using a five-minute HRV assessment.
The back school program was provided by experienced physiotherapists on an individual basis. It focused on the physical aspects, such as increase in physical capacity or ergonomics, and behavioral aspects, which could be cognitive behavioral- or acceptance-based approaches. The duration was 12 weeks, two times per week in a cardio fitness setting, for a total of 24 hours in the BS group.
Training in heart coherence and the self-regulation techniques was provided six times, once per week in an individual setting with one hour per meeting, for a total of six hours. Patients were trained in a therapy setting and practiced using the techniques at home. BS-HCT followed a standardized certification program protocol by the HeartMath Institute (HeartMath Interventions Program). The first HCT sessions were focused on learning the basic self-regulation techniques. After the patients learned the basic techniques, they were exposed to stressors by focusing on individualized negative feelings and emotions, including their pain.
Both groups improved significantly on NRS pain, RMDQ, PDI and most of the Rand 36 subscales. On physical functioning, the BS+HCT group improved significantly more than the BS only group (p = 0.02). Significant correlations (r=0.39 and r=0.48) were found between increased heart-coherence scores and reduced PDI pain and RMDQ disability scores, but not with other variables. Providing BS-HCT was more effective on physical functioning than the BSonly program was.
Self-Regulation for Caregiver Settings
In recent years, an increasing number of studies on stress have focused on professional caregivers. Affected professionals speak of burnout to define a state of emotional and physical exhaustion caused by the stressful demands of their daily work. The study of these two conditions has been developed in areas of high demand for services such as care for people with dementia. Because dementia is a progressive, disabling and long-term neurodegenerative disease, the risks of being exposed to chronic stress situations for both professional and family-member caregivers is very high.[286] Many studies show the consequences of professional stress, both emotional and physical, that can cause communication problems in the team and families and affect the general welfare of the person. [287] Improving the ability of caregivers to effectively meet the challenges of their daily work is valuable not only for institutions because they will have workers who are less stressed and healthier, but also for people receiving care.[288]
A study conducted in three long-stay nursing homes for elderly people located in different cities in Spain examined the outcomes of providing stress-management intervention based on HeartMath’s selfregulation techniques and heart-coherence training with the emWave PSR (now called emWave2) in a group of nursing professionals and family caregivers of elderly patients with dementia.[289] The conceptual nursing model that guided the implementation of this study was Jean Watson’s theory of Human Care.[290] Watson’s theory emphasizes the importance of taking care of oneself, colleagues or family and others as a means of achieving a more healing environment.
Participants included 42 professionals (67.9% certified nursing assistants) and 32 family-member caregivers. The only exclusion criterion was subjects with sensory or cognitive impairment that prevented them from understanding the training content. A number of socio-demographic variables were collected, including age, sex, occupation, education level, medical history, drug use, years of caregiving and information about people under their care, such as degree of dementia.
The degree of stress and burnout for the professional caregivers was assessed with the Maslach Burnout Inventory (MBI), which has three primary subscales: emotional exhaustion, depersonalization and personal accomplishment at work. For family caregivers, the scale used to assess overload was the validated Spanish version of the Zarit Burden Inventory, which reflects the level of overload a person is experiencing. For measurement of heart coherence, the emWave Pro was used to assess participants’ coherence levels at pre- and three-months-post-training during resting state and during a period in which they were asked to relax. In addition, at the end of the workshops, participants’ filled out questionnaires on stress and overload, and heart-coherence measures were obtained.
The self-regulation skills training was conducted in workshop style with groups of 10 people, without differentiating between professional and family caregivers. The workshops were provided in one-hour weekly sessions, over a three-month period. Only people who attended more than 80% of the workshops were included in the analysis. The results of an ANOVA analysis of the professional caregivers three months after the training found a significant reduction in the MBI scales for emotional exhaustion and improvement in performance. The depersonalization scale was not significantly changed. In the family caregivers group, the Zarit scale results were not statistically confirmed after a Bonferroni correction (p = .04). A noteworthy finding among family caregivers was a high percentage of hypertension (43.7%), insomnia (28.7%) and anxiety (31.8%), each of which required taking of at least one drug on a daily basis. In professionals, the most prevalent issues were sleep problems (27.8%) and muscular or mechanical (47.6%) problems. Regarding heart-coherence scores, at baseline 58.7% of all participants (n = 71) had low heart-coherence scores. At post assessment, 86.4% of participants had high heart coherence, with significant increases over the baseline values.
The authors concluded that the main objective of this work was to reduce the levels of stress and overload through increased psychological control and increased heart coherence in a group of professionals and caregivers of people with dementia. The results suggest that the intervention achieved the main objective.
Physician Stress Reduction
Given the nature of their occupational duties and environment, physicians often experience work-related stress that may lead to burnout, depression and substance abuse, as well as impaired professional performance. These may be indicated by medical errors, reduced attentiveness or caring behavior toward their patients and other staff members. Physician wellness has been increasingly linked to the quality of patient care, yet the attention that physicians pay to self-wellness often is suboptimal.
A randomized controlled study conducted by Jane Lemarie and colleagues at the University of Calgary with 40 physicians (23 male and 17 female) from various medical practices (1 from primary care, 30 from a medical specialty and 9 from a surgical specialty) was conducted to assess the efficacy of HeartMath selfregulation skills training supported by HRV coherence training (emWave2) for reducing physician stress.[291] Participants in the intervention group were given an HRV coherence training device and were instructed in how to use it. They also participated in an individual training session to learn the Quick Coherence selfregulation technique and were instructed to use the HRV device during the study for five minutes at least three times daily. A research assistant contacted each participant in the intervention group twice weekly to measure stress, heart rate, blood pressure and overall well-being to document adherence to using the stress-management techniques and to record a three-minute HRV session using the emWave Pro system. Participants in the control group received a brochure describing the provincial physician wellness support program and were contacted twice weekly by a research assistant to measure stress, heart rate, blood pressure and overall well-being.
The primary outcome, stress, was assessed with a multiple-item scale developed by the research team, which measured global perceptions of stress and captured occupation-specific stress that is particularly relevant to physicians. The survey included 15 items from the Perceived Stress Scale and 25 items from the Personal and Organizational Quality Assessment – Revised (POQA-R) questionnaire for anxiety, anger, physical symptoms of stress and work-related time pressures. The final 40-item instrument was validated through confirmatory common factor analysis. Pre-intervention data was compared to data collected 28 and 56 days later.
The analysis of the data at day 28 showed that the mean stress score declined significantly for the intervention group (change -14.7, standard deviation [SD] 23.8; p = 0.013) but not for the control group (change -2.2, SD 8.4; p = 0.30). The difference in mean score change between the groups was 12.5 (p = 0.048). The lower mean stress scores in the intervention group were maintained during the trial extension to day 56. After the assessment at day 28 the control group received the same intervention, after which mean stress scores were significantly lower at day 56 (change -8.5, SD 7.6; p < 0.001).
The authors concluded that HRV coherence training along with practice of a self-regulation technique may be a simple and effective stress-reduction strategy for physicians.
Medical Error Reductions
Another study conducted with a large chain of retail stores that had in-store pharmacies employing 220 pharmacists across multiple locations found a reduction in medical errors ranging from 40% to 71%, depending on the store location.[292]